
 Failure to diagnose is the most common medical error in the practice of emergency, urgent care and primary care medicine. Spinal epidural abscess (SEA) is one of the most difficult conditions to diagnose, but there are common threads among failure to diagnose spinal epidural abscess cases. This case is presented to provide perspective and to increase our vigilance for catching this disabling and possibly even fatal diagnosis.
Failure to diagnose is the most common medical error in the practice of emergency, urgent care and primary care medicine. Spinal epidural abscess (SEA) is one of the most difficult conditions to diagnose, but there are common threads among failure to diagnose spinal epidural abscess cases. This case is presented to provide perspective and to increase our vigilance for catching this disabling and possibly even fatal diagnosis.
ED Visit #1, Day 1
Physician History: A 40-year-old woman presented to the ED at 0400 with the complaint of right lower back pain, rated a 7 out of 10. It was worse with cough and improved with sitting. There was no recent trauma and no apparent precipitating event. She told the emergency physician that she had weakness in her legs, but that it was “unchanged” and nonfocal. Her legs felt “very heavy.” She said she had similar symptoms in the past that resulted in aspiration pneumonia 3 years ago; that required surgery to “drain her lungs.” She said she had an ongoing cough and shortness of breath that had not changed that she felt were related to smoking.
Review of Systems: No problem with gait; neuro review was negative for weakness, lightheadedness, numbness and headaches. No urine or fecal incontinence. No numbness or tingling.
Triage Vital Signs:
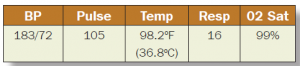
Physical Exam: The physician noted: “Vital signs are normal.” The patient was morbidly obese.
Musculoskeletal: Normal ROM. No tenderness. Lumbar area exhibits tenderness (drawing of low back with arrow pointing to just above the iliac crest).
Neuro: Alert, no cranial nerve deficit. Coordination normal. There were no motor, sensory, reflex or gait exams.
ED Course: WBC 15.7; glucose 236. CXR negative. Patient was treated with an albuterol nebulizer.
Medical Decision-Making: Patient is concerned about pneumonia. The differential diagnosis includes pulmonary embolism, pneumonia, pleural effusion, UTI, back strain. CXR unremarkable. Patient condition stable and will be discharged home. Instructed patient to follow up with her primary care physician for weakness in her legs. Prescribed a nebulizer for SOB and a Z-Pak.
RN Notes. “Pt. reports mid back pain X 3 days, right > left, increasing with cough and laying down. Clear sputum. History of same pain, diagnosed with pneumonia at that time, 3 years ago. She denies shortness of breath and chest pain.”
ED Visit #2, Day 4
On Day 4 the patient returned to the same ED.
Physician History: 40-year-old female with hypertension, diabetes with neuropathy, with back and abdominal pain. Bilateral low back pain began 1 week ago and radiates into her lower abdomen. Acutely worsened and became constant today at 2:00 pm. Associated urinary frequency, unable to lay flat. Similar pains a few years ago; diagnosed with pneumonia. Concerned about kidney infection, stones or nerve impingement in back. No relief with NSAIDS or with antibiotics given a few days ago. “Denies any associated numbness, tingling, urinary or bowel incontinence, or saddle anesthesia.”
Review of Systems: No focal weakness or loss of consciousness
Physical Exam:
No distress.
Lungs: Mild wheeze, otherwise clear to auscultation
Heart: NSR
Abdomen: Non-tender, +right CVA tenderness
Neurologic: Moving all extremities, no gross neuro deficit
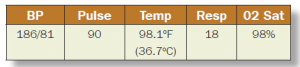
ED Course: Normal white count, glucose 377. UA negative. Renal CT negative. Patient received IV fluids, Toradol, insulin and Dilaudid for continuing pain.
Medical Decision-Making: Felt better after second round of meds. Advised to follow up with her primary care physician on Monday and to possibly pursue MRI should she not improve. Additionally, she may have a UTI, which is masked by current or recent antibiotics. Therefore, she will be provided with antibiotics at discharge to treat for possible UTI or pyelo. She was treated with Bactrim, Toradol and Flexeril.
PA Clinic Visit #3, Day 7
PA Exam: 40-year-old complaining of acute and chronic atraumatic back pain for several days. Patient states she does not know why she did not call her clinic physician today. Pain is 7 out of 10, nonradiating and constant. Worse with ambulating or range of motion. Denies trauma, numbness, tingling of bilateral lower extremities. No loss of bowel or bladder function; no saddle anesthesia or loss of sensation or strength bilateral lower extremity. No fever, weight loss, malaise, night sweats, diaphoresis or shortness of breath. No chest pain, nausea, emesis, recent or long-term steroids, or osteoporosis.
Review of Systems: Otherwise negative.
Physical Exam:
On physical exam, the PA noted musculoskeletal exam “normal range of motion.”
Neurologic Exam: He noted: “She is alert.”
Clinic Course: “Patient had paraspinous tenderness at L3-5 without midline spinous process tenderness. I did not order imaging due to no new trauma and patient is neurovascularly intact on physical exam. Patient was observed ambulating to and from the bathroom. Epidural abscess was considered however excluded based on no history of fever and no history of IV drug abuse.”
Patient was discharged on Ativan and Dilaudid. Discharge instructions: Return for leg weakness, numbness, fever, chills, or bowel or bladder incontinence.
ED Visit, Visit #4, Day 7
The patient presented to the emergency department later that same day. The physician noted in his history of present illness the patient had been discharged earlier today, presents after falling in driveway. She has lumbar back pain for 9-10 days, radiating down both legs. The physician addressed the period of time following discharge from the PA clinic. She drove home; she was unable to feel her legs and ended up falling out of the car onto the driveway.
Her mid lumbar back pain worsened this morning when she was walking in her kitchen. She noted a snap and had sudden lumbar back pain that radiated to her legs bilaterally with associated numbness. She was able to walk to the bathroom without difficulty and urinate; however, she could not get up from the toilet. States that later she urinated on herself and was not aware of this.
Review of Systems: Otherwise negative.
Physical Exam:

Back Exam: Left lumbar tender, unable to lift legs. Unable to dorsiflex great toes bilaterally or move legs. Denies sensation in both legs, but able to sense pinprick. Normal patellar DTRs; absent Achilles DTRs; upgoing Babinski on the right, downgoing on the left.
Neurologic Exam: Bilateral upper and lower extremity 5/5 strength, no gross neuro deficit.
Sinus tachycardia at 124. Urinalysis: elevated sugar. Lactate: 1.0. White blood cell count: 17,000.
CMP: Bicarbonate 19; glucose 285. Sed rate: 43.
MRI of the lumbar spine T12-L5 showed L5-S1 disc desiccation and mild loss of disc height as well as a focal posterior midline protrusion, which indents the thecal sac; however, it does not significantly narrow the central canal and degenerative joint disease.
ED Course: Reviewed the differential diagnosis and reviewed labs. Noted that the patient could not ambulate, was felt to have possible pneumonia, and was started on antibiotics and transferred to inpatient at an outlying hospital. Diagnosis: acute lumbosacral back pain, inability to ambulate, pneumonia.
Hospital Course, Day 7
The physician at the receiving hospital documented an admission history and physical exam. He documented significant neurologic deficits and the prior “unremarkable MRI.” There was uncertainty about the cause, and there was a plan to ask for a neurologic consultation.
Hospital Course, Day 8
The next day the patient was seen by a neurologist who documented in a progress note. He noted: “Sensory exam is noticeably different from yesterday’s exam.” He noted the patient did not appear to be making an effort when he asked her to flex at the hips and that there were a number of discrepancies in her exam. He concluded, “Although patient may have a lumbosacral radiculopathy nerve process, I believe her presentation is suggestive of embellishment or functional disorder.”
Hospital Course, Day 9
The patient’s neurologic condition continued to deteriorate. On day 9, she had an MRI that showed an epidural mass from C6-T10, which was initially called a hematoma by the radiologist. On further review, she was found to have a large SEA, which was reported to the hospitalist. There is an operative note from later in the day that describes evacuation of the abscess.
This is a relatively recent case, and the patient’s outcome is unknown. It is also not known whether there is any litigation currently pending in the matter.
Failure to Diagnose Spinal Epidural Abscess - Discussion
Visit #1.
 There are several issues worthy of note from the first emergency department visit.
There are several issues worthy of note from the first emergency department visit.
- The patient presented with back pain without trauma or some other precipitating event. Although SEA can be an incredibly difficult diagnosis to make, a patient presenting with back pain without a precipitating event should create a suspicion for a perispinal process.
- This presentation required a complete neurologic examination. As a general rule, the practitioner should perform a complete examination of the relevant organ system. In this case, the neurologic system was one of the relevant organ systems. The practitioner did not address motor, sensory or focal deficits. The practitioner did not specifically address the presence or absence of cauda equina syndrome. This was an inadequate neurologic exam.
- The patient presented to the emergency department with tachycardia; there was no repeat set of vital signs, and the patient went home with tachycardia. This is a common finding in emergency department medical care. In retrospect, it is often one of the physical findings in cases of failure to diagnose that could or should steer the practitioner toward the correct diagnosis.
- The practitioner anchored on the possible pneumonia diagnosis and prematurely closed the decision-making thought process. The patient’s pre-existing conditions - morbid obesity, diabetes and hypertension - significantly complicated decision-making in this case. However, the key point is that the patient had new back pain without a precipitating event, tachycardia, and an elevated white count, and she did not have signs or symptoms of pneumonia. The medical decision-making section indicates a thought process related to pneumonia, which was treated on discharge with antibiotics. It may not have been possible to diagnose an epidural process during this first visit, but it is clear at discharge that the physician settled on an incomplete explanation for the patient’s presentation.
Visit #2
- Visit #2 complicated the analysis. The vital signs had normalized and the patient developed frequency of urination. The practitioner addressed the neurologic system in both the review of systems and in the physical examination, indicating that there were no focal neurologic deficits.
- The return visit, or bounce-back, should always raise a red flag. At a minimum, it is unusual that on visit #1 the patient was complaining of back pain and heavy legs and was then treated for possible pneumonia. Then she returned on visit #2 with a focus on her urinary tract with possible infection or pyelonephritis. That thought process alone should cause significant concern, particularly since there was no actual laboratory or imaging evidence of urinary tract infection or other pathology.
Visit #3
- The visit to the physician assistant is interesting. The documentation indicates a thorough review of systems related to the neurologic system and a good neurologic examination. In addition, it appears that the PA considered the possibility of an epidural abscess. However, in his mind, he ruled that out because there was no history of fever or neurologic deficit. On the other hand, since the patient drove home and was unable to support herself getting out of the car, it is hard to believe that perhaps 30 minutes earlier she had a completely normal neurologic examination of the lower extremity.
- In addition, there was again no repeat of the abnormal pulse in the face of tachycardia. And there was no mention or recognition of the fact that the patient was tachycardic. Although it is easy to write off tachycardia as related to anxiety or pain, it is critical for practitioners to recognize that in the failure-to-diagnose world, tachycardia is often an important physical sign of early sepsis and pulmonary embolism. In failure-to-diagnose cases of both entities, tachycardia is a common and often overlooked finding.
Visit #4
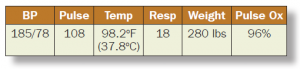
- The patient presented to the emergency department with complaints that indicated a neurologic process was underway. She had been unable to feel her legs and fell out of the car onto the driveway. She was unable to get up from the toilet and she urinated on herself. The patient’s pulse at triage was 119. Regarding the back exam, the physician said the patient was unable to lift her legs, unable to dorsiflex the great toes bilaterally or move her legs. On the other hand, he noted in the neurologic examination that the patient had 5/5 strength upper and lower extremities and no gross neurologic deficit. The MRI (limited to the lumbar area) revealed loss of disc height and focal posterior midline protrusion, which did not significantly narrow the central canal. These imaging results don’t explain the patient’s complaint.
- The emergency physician again anchored on pneumonia as a possible diagnosis and ordered appropriate antibiotic therapy for that diagnosis.
Spinal epidural abscess can be a very difficult diagnosis to make. It is simply not fair to say that the diagnosis should have been made during visit #1 or visit #2. The patient never complained about fever or shaking chills. However, the patient complained during visit #1 of back pain without a precipitating cause, a lower extremity complaint that could have had a spinal etiology, tachycardia, and an elevated white blood cell count. Perhaps the physician was caught by the search satisficing heuristic. With a normal chest X-ray, no purulent sputum, and no fever, his first consideration was pneumonia; that is, once satisfied that the search for a diagnosis may be over, the physician stopped the diagnostic thought process. The diagnosis of pneumonia simply does not explain the patient’s low back and lower extremity symptoms. Tachycardia was never addressed in the physician’s medical decision-making, and the vital signs were never repeated by nursing.
Many cases of failure to diagnose SEA are complicated by MRI imaging at the wrong spinal level. There is absolutely a common thread in failure to diagnose SEA cases. Practitioners typically order an MRI of the lumbar spine when, in fact, the abscess is at a higher level in the spine or is at multiple levels in the spine. Review of the literature does not provide any standard with regard to which levels of the spine should be imaged when considering the possibility of a spinal epidural process. There have been efforts to come up with a prediction rule with regard to spinal epidural abscess and consideration of pan-spine MRI. However, there is simply not enough literature to justify that as a recommendation.
It appears that the physician assistant simply missed a neurologic deficit, although that is in part conjecture. What is striking is his thorough neurologic documentation that suggested the patient had no neurologic problems. Perhaps this is a result of EMR overuse syndrome; in other words, it may simply have been easy to check a box and get a completely normal neurologic system documented through the electronic medical record system.
We present this case not to point a finger at any particular individual or visit, but rather to continue to raise awareness of the failure to diagnose problem in general and to take another look at the failure to diagnose spinal epidural abscess specifically. It is through this type of analysis, a cognitive autopsy if you will, that we can learn to recognize the red flags in cases of concern in the failure to diagnose arena.
Have you experienced an interesting case recently? Share with The Sullivan Group and we'll review for potential future inclusion in our Clinicians Corner.

