
 Physician workflow frustrations are cited by several studies as a significant contributing factor to physician burnout, an epidemic estimated to impact 51% of the physician population according to Medscape’s 2017 study. Because burnout can be tied to risks in patient safety, improvements in physician workflow are key components in the patient safety movement.
Physician workflow frustrations are cited by several studies as a significant contributing factor to physician burnout, an epidemic estimated to impact 51% of the physician population according to Medscape’s 2017 study. Because burnout can be tied to risks in patient safety, improvements in physician workflow are key components in the patient safety movement.
Over the decades, physicians have worked with various medical record documentation styles. While this evolution is thought to improve patient care with each step, the majority of physicians and health systems have yet to maximize the potential of their documentation to improve patient safety. Moreover, each evolution might also be cited as being more complicated and time consuming for the physician, thus adding to their workflow frustrations.
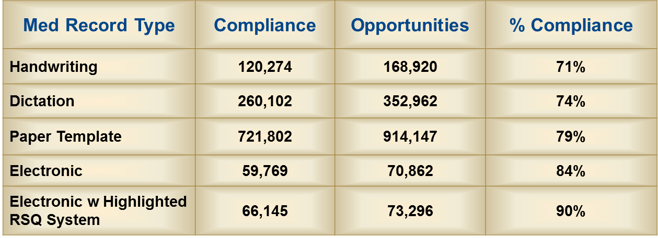
A study published in the Annals of Emergency Medicine1 analyzed various physician documentation methods and their potential impact on compliance with key Risk, Safety, Quality indicators (RSQ® Score). The study reviewed the strength of documentation for 100,000 high-risk emergency department visits across the United States.1 For each medical record type, a total number of documentation opportunities were identified that could impact the risk, safety and quality of the encounter. Records were then reviewed to identify how the documentation complied with the completion of those opportunities. Higher compliance levels indicated a safer patient experience according to the index.
Comparing Documentation Methods
Handwritten Notes: RSQ® Score 71%
For those that have reviewed medical malpractice cases, it is no surprise that this documentation style results in the most exposure to medical professional liability claims. Simply writing notes – often illegible notes - on a blank paper provides no clinical content to serve as a guide for documentation and decision-making. Although this was the primary form of documentation many years ago, in some organizations it has returned to the physician workflow due to remarkably inadequate clinical applications within the enterprise EHR systems that don’t align with a physician’s workflow.
Dictation: RSQ® Score 74%
Akin to the handwritten note, dictation does not provide enough visual guidance to increase documentation compliance on key elements in the diagnostic process, including the history, physical, reevaluation and discharge. The use of Dictation as part of the physician workflow can be very helpful in creating a detailed narrative that supports each unique patient encounter. A note that reads well does play well in court. However, with an RSQ® Score of 74%, the sole use of dictation presents many missed opportunities to document key clinical elements that correlate with an increase in exposure to litigation in the event there is an adverse outcome (e.g., Missed AAA: Documenting absence or presence of pain radiation in abdominal pain patient over 40).
Paper Templates: RSQ® Score 79%
 Perhaps because of expensive transcription or dictation services or as a result of a greater desire to create efficiencies, paper templates appeared in the 80s/90s with rapid adoption. This is a remarkably quick, easy way to create a medical record. Despite many contrary beliefs, they are still used widely by emergency departments and private practices across the U.S. Although paper templates have many strengths, most of the large paper template vendors did not have strong enough clinical risk content in their product to facilitate strong medical-legal documentation. However, our work with many clients in the early 2000s did lead to modifications to paper templates that resulted in a dramatic improvement in their risk profile.
Perhaps because of expensive transcription or dictation services or as a result of a greater desire to create efficiencies, paper templates appeared in the 80s/90s with rapid adoption. This is a remarkably quick, easy way to create a medical record. Despite many contrary beliefs, they are still used widely by emergency departments and private practices across the U.S. Although paper templates have many strengths, most of the large paper template vendors did not have strong enough clinical risk content in their product to facilitate strong medical-legal documentation. However, our work with many clients in the early 2000s did lead to modifications to paper templates that resulted in a dramatic improvement in their risk profile.
Electronic Medical Records (EMRs): RSQ® Score 84%
The desire to innovate, advance and harness the perceived efficiencies in coding and billing largely drove the adoption of EMRs. Many physicians or providers reading this probably think it is impossible that an EMR led to a higher RSQ® Score than the previously mentioned documentation styles. However, it is important to note that the EMR systems that were used during the time of our analysis were largely built by clinicians for clinicians/best in breed systems. This includes EMRs such as Ibex (now Picis), MEDHOST EDIS, Wellsoft, etc. These specialized systems did provide strong clinical content in their templates and supported the workflow of emergency physicians. Unfortunately, the Meaningful Use movement pushed many hospital systems to purchase enterprise EHR systems (Epic, Cerner, Meditech, McKesson, etc.); as a result, we are finding more physicians reverting to the aforementioned documentation styles (dictation or typing) in addition to new shortcuts (dotphrases, macros, etc.) that are very susceptible to fraud and abuse.
EMR with Risk Mitigation Module: RSQ® Score 90%
Risk Mitigation Module (RMM) is a library of risk and safety content programmed into the EMR. It provides an integrated clinical decision support system within the EMR. Based on our analysis, this documentation style provides the greatest amount of protection to the patient, the provider and the organization against adverse events and litigation. Although the first iteration existed in 1999 with Ibex (now Picis), the adoption of electronic documentation systems with a greater focus on clinical risk management content has increased dramatically. For the sake of patient safety, we hope to see a continuous growth in the adoption of risk-enhanced EMR systems, either through the aid of outside vendors or the hospital’s internal process.
References
- Hafner JW, Parrish SE, Hubler JR, Sullivan DJ/University of Illinois College of Medicine at Peoria, Peoria, IL; The Sullivan Group; Cook County Hospital/Rush Medical College. Quality in Emergency Department Care: Results of the Sullivan Group’s Emergency Medicine Risk Initiative National Audit. Abstract # 211 in Annals of Emergency Medicine, Vol. 46 Issue 3; September 2005.
